Carpal-Tunnel-Syndrom (CTS)
Causes and symptoms | Diagnosis | Conservative treatment | Surgical treatment | After the treatment
Carpal tunnel syndrome is one of the most common conditions in hand surgery. In 1932, carpal tunnel syndrome (CTS) was described by Dr Learmont (USA) and treated with surgery.
The carpal tunnel is bordered by eight carpal bones and covered by a thick band structure (the flexor retinaculum). In addition to the nine finger flexor tendons, the median nerve also runs through this narrow tunnel. This is responsible for the strength of the muscles of the ball of the thumb and for feeling in the thumb, index, middle and half of the ring fingers.
Constriction of the median nerve in the carpal tunnel can damage the nerve. This can have various causes, including the following: Anatomical narrowness, inflammation and swelling of the flexor tendon sheaths, pregnancy, forearm fractures, diabetes mellitus, polyarthritis, infections in the wrist area, hypothyroidism. Statistics indicate that carpal tunnel syndrome occurs in up to 14% of the population. It is three times more common in women than in men. People between the ages of 40 and 60 are most commonly affected. The dominant hand usually shows symptoms first. According to a large-scale study, working on a computer is not responsible for the frequent occurrence of carpal tunnel syndrome.
Symptoms
Often the first symptom is numbness of the hand at night and walking with tingling in the fingers. Pain at night, which radiates up to the arm and shoulder, can also be the first symptom. Initially, this pain at night can usually be alleviated by shaking hands the hands. With continued pressure on the nerves, weakness of the hands and muscle loss in the ball of the thumb can occur. This is the only change that is externally visible. The symptoms in the fingers can progress to include numbness and fine motor impairment. This can go as far as damage to the nerve fibres, which can mean that the pain subsides. Often symptoms such as tingling can be triggered by the position of the wrist, such as when reading a newspaper, driving a car, cycling, or supporting the hand on a surface.
In addition to noting the symptoms described, a careful clinical examination is of great importance for the diagnosis. The focus is on testing the comparative finger sensitivity using the following tests:
- Hoffmann Tinel sign: Tapping the median nerve on the palmar side of the wrist triggers a tingling electric shock sensation in the median nerve distribution (can be triggered in approx. ¾ of cases).
- Phalen test: If the wrist is flexed at 60º, tingling and/or electric shock sensations occur after approx. 60 seconds.
- Reverse Phalen test: The same symptoms occur as with the Phalen test when the wrist is extended at 60°.
- Bottle sign: Due to the muscle weakness in the ball of the thumb, a bottle cannot be properly enclosed by the thumb and fingers.
NEUROPHYSIOLOGICAL INVESTIGATIONS
Neurophysiological examinations can also provide information about the condition of the nerve. These examinations are carried out by neurologists.
- EMG (electromyography): Electromyography can be used to investigate whether more nerves or muscles are damaged. The location of the damage can thus be determined.
- ENG (Electroneurography): Electroneurography measures how quickly the median nerve transmits a stimulus.
- Ultrasound: Ultrasound can also be used to identify compression (narrowing) of the median nerve.
If the examinations show that the symptoms cannot be attributed to carpal tunnel syndrome, other causes such as polyarthritis of the finger and/or wrist or a circulatory disorder of the hand must be investigated.
TREATMENT OPTIONS
In mild forms, carpal tunnel syndrome can be treated conservatively. Wearing special splints that fix the wrist in a neutral position can alleviate the symptoms at night in particular. Cortisone injections into the carpal tunnel can reduce swelling of the tendon sheath tissue and thus the pressure in the tunnel. But injections into the carpal tunnel are not without risk. If the cortisone is injected into the nerve, it can be severely damaged. Taking cortisone in tablet form can also be useful in the short term, especially for severe acute carpal tunnel syndrome. Around 70% of people with carpal tunnel syndrome initially respond to conservative therapies. Most of the symptoms return after a year at the latest and 50% then need surgery.
The aim of the surgical procedure is to relieve pressure on the nerve and improve the blood vessels that supply it. In the open procedure (Figures 1 and 2), an approx. 3–4 cm incision is made in the palm of the hand providing direct access to the flexor retinaculum, which is cut. The visible median nerve is protected. This provides decompression of the carpal tunnel and relieves pressure on the nerve. Figure 1
Figure 1
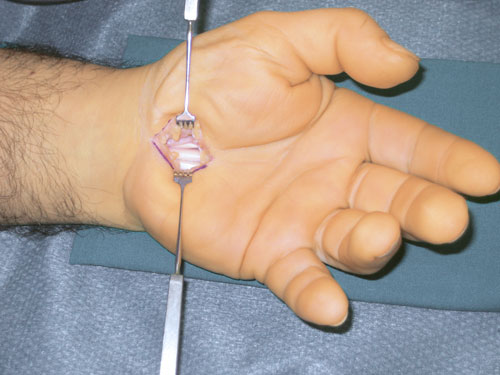 Figure 2
Figure 2
The procedure takes place in what is called a bloodless field. The blood flow to the arm is interrupted and the bloodless field is maintained with a cuff around the upper arm. The operation is carried out using a surgical loupe (magnifying glasses).
The endoscopic procedure was introduced over 15 years ago. This method is used because of the smaller scars and faster recovery of hand function. However, this procedure resulted in a higher rate of incompletely cut tunnels and thus a higher complication rate. Comparative studies have shown that the endoscopic and open techniques have practically identical results. At the Pyramid Clinic we use the open procedure almost exclusively. The scar is nearly invisible after about 6 months. Fortunately, the general risks of this procedure (e.g. infection, subsequent bleeding, damage to vessels and nerves) are rare. The surgery can be performed under regional anaesthetic. A general anaesthetic is only required in special cases.
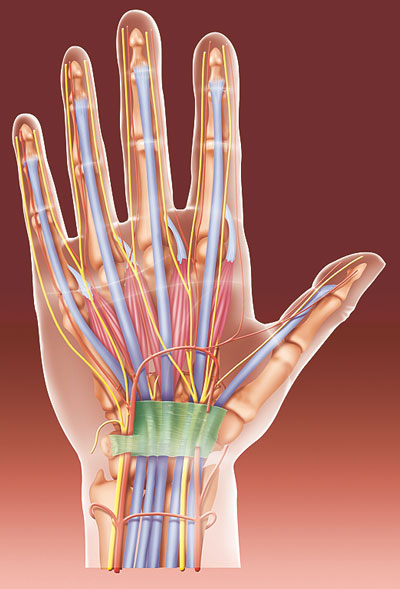
Figure 3: During the surgery for carpal tunnel syndrome, the ligament running over the pinched nerve (green in the image) is cut, thus indirectly relieving pressure on the nerve. This is what enables recovery.
A brief period of immobilisation of one to two weeks is the rule. Splint fixation is not mandatory and is at the surgeon’s discretion. When to return to work depends on the type of activity: light office work can be resumed after a few days, manual workers (e.g. construction workers) can resume work after 6 to 12 weeks. Early functional treatment, exercises at home and elevating your hand in the first few days prevent swelling and finger stiffness.
Recurrence after surgery is extremely rare and usually only occurs if there is incomplete transection of the retinaculum or significant inflammation of the tendon sheaths.
If the disease has been present for a long time, the nerve may take months to fully recover. With significant pre-existing damage to the nerve (from a high level of compression over a long period), there may not be a full recovery. In these cases, surgery can also be useful to prevent the nerve damage from progressing. The final result in terms of recovery of strength and/or sensitivity takes around 6 to 12 months.
Author: Dr Markus Strickler, FMH Specialist in Surgery, specialist field: Hand surgery
FACTS AND FIGURES
![SURGICAL PROCEDURE]()
SURGICAL PROCEDURE
30 minutes, under local or regional anaesthetic
![SURGICAL PROCEDURE]()
HOSPITAL STAY
![AFTER THE TREATMENT]()
AFTER THE TREATMENT
Bandage for 1 week, rest for around 4 weeks, then increasing use possible
![TIME OFF WORK]()
TIME OFF WORK
Resume work after 2 to 3 weeks
![Sport]()
Sport
![READY TO SOCIALISE]()
READY TO SOCIALISE
![COSTS]()
COSTS
Cost coverage must be requested from your health insurance company
TECHNICAL TERMS
Synonyms/Abbreviations for Carpal Tunnel Syndrome:
- CTS
- Median nerve entrapment syndrome
Median nerve:
Nerve that runs parallel to the flexor tendons of the fingers and is responsible for the strength of the muscles of the ball of the thumb and the feeling of the thumb, index, middle and half of the ring finger.
Retinaculum:
Roof of the carpal tunnel