Causes and symptoms | Diagnosis | Treatments | Consultation & second opinion
What is the meniscus and where is it?
The meniscus is a crescent-shaped piece of cartilaginous connective tissue with a triangular cross-section. We have two menisci per knee: one on the inside and one on the outside of the knee.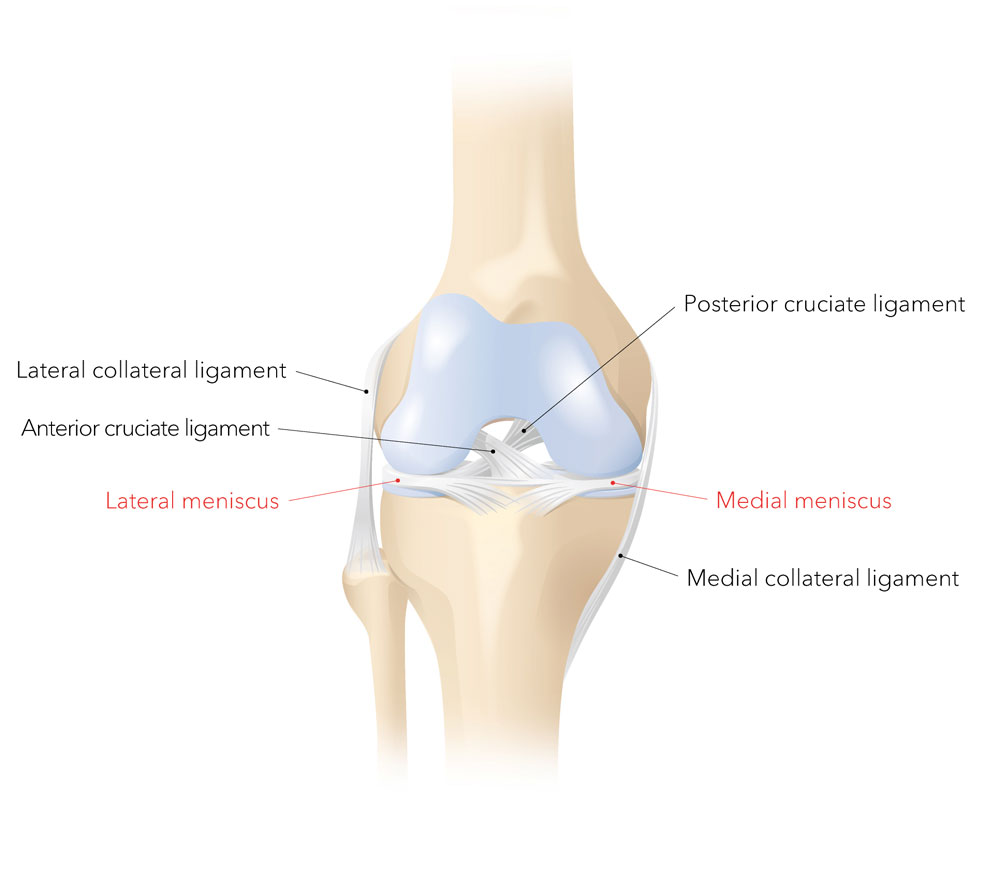 The meniscus acts as a buffer between the bones of the thigh and the lower leg, protecting the cartilage. The menisci also evenly transfer the force from the thigh to the lower leg.
The meniscus acts as a buffer between the bones of the thigh and the lower leg, protecting the cartilage. The menisci also evenly transfer the force from the thigh to the lower leg.
A sharp pain in the knee joint when carrying out certain movements indicates a problem with the meniscus. Most patients report immediate, stabbing pain, typically on the inside of the knee joint following rotation of the upper body with the lower leg stationary, or on squatting. Some people also describe locking, effusion, snapping or restriction of movement. The meniscus itself does not hurt because, like the cartilage, it does not have any nerves. However, a torn meniscus can irritate the joint capsule as the knee twists and flexes, triggering a sharp pain and leading to effusion. In the worst case, fragments of the meniscus can cause the knee to lock.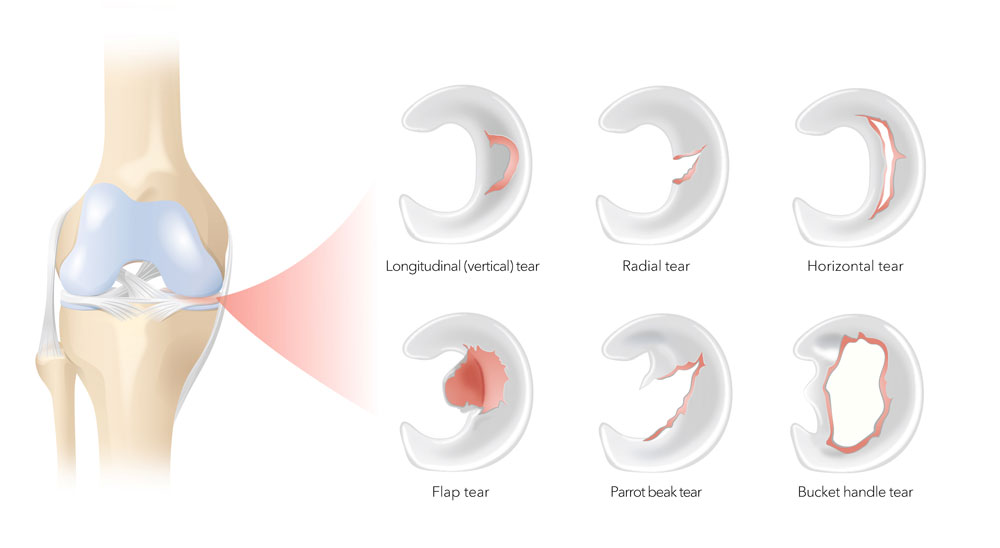
In most cases, a thorough clinical examination is sufficient to diagnose a meniscus tear. The sharp, movement-dependent pain is triggered as part of the examination. Magnetic resonance imaging (MRI) provides further information on the size, type and localisation of the torn meniscus and other cartilage damage in the knee joint.
A meniscus tear can be treated either conservatively or with meniscus surgery. The method chosen depends on the age and needs of the individual and the type (accident-related or degenerative), localisation and extent of the meniscus tear. Any other injuries in the knee joint also play a role. These must be discussed with the patient in detail.
Conservative therapy
You can live with a meniscus tear, but you should avoid rotational movements and vigorously flexing the knee joint. You can read more about this in the NZZ article on “Exercise instead of surgery” (in German)
Unfortunately, the meniscus does not heal by itself. Any of these movements can cause the tear to grow larger, causing new stabbing pains. In some cases, a piece of the torn meniscus can break off and catch in the joint, causing the knee to lock. If this happens, quality of life is severely impacted. To treat this, meniscus surgery is required in certain cases.
Meniscus surgery
Meniscus surgery is usually advised in the following cases:
- For young patients who play sport
- If there has been no improvement in movement-related pain, despite conservative therapies
- If mechanical discomfort such as entrapment and locking does not disappear
Meniscus surgery can include the following procedures:
- Meniscus repair
- Removal of a piece of torn meniscus
- Meniscus replacement (in very rare cases)
The procedures are all minimally invasive and are performed using arthroscopy. The video camera and instruments are inserted into the knee via two small incisions of around one centimetre each on the right and left of the patellar tendon.
Meniscus repair
The blood vessels lead from the joint capsule into the outer meniscus and supply the outer third of the meniscus. The remainder, i.e. two-thirds of the meniscus, does not have a blood supply. The cells here are fed directly by the synovial fluid. The outer meniscus is more mobile than the inner meniscus, which is fused with the joint capsule and the inner knee ligament. The ruptured meniscus tissue is sutured to attach it to the healthy, perfused part of the meniscus as well as to the joint capsule, so that the ruptured meniscus tissue can be supplied with blood and is thus able to heal.
Only a small proportion of meniscus tears can be sutured, such as certain longitudinal tears near the joint capsule. The location, quality and overall blood supply of the knee play a role, as does the person’s age. The younger the person is and the better the blood supply to the meniscus, the better the cure rate and, therefore, the greater the success rate.
In most cases the surgeon can only see during the arthroscopy whether a meniscal suture would be possible and appropriate. Non-healing of a meniscal suture (failure rate) can be up to around 20%. Surgery must be performed again in these cases. This involves either removing the suture and the torn part of the meniscus or placing a new suture in case of rupture. Meniscal sutures in fresh (accident-related) meniscus tears heal better than in older (chronic) tears. If there are multiple knee injuries (e.g., cruciate ligament rupture), all of these must be corrected at the same time.
Facts and figures
![Operation]()
Operation
The procedure takes around 60 minutes
![Operation]()
Length of stay at the clinic
![After the treatment]()
After the treatment
Post-operative use of crutches to protect the knee for 4 to 6 weeks, physiotherapy for around 3 months and no flexing the knee greater than 90 degrees for 6 weeks
![Back to work]()
Back to work
No office work for around 2 weeks, no strenuous physical activity for about 8 weeks
![Sport]()
Sport
Knee-friendly sports such as swimming, cycling, fitness etc. from about 2 months after surgery; contact sports such as football or stop-and-go sports such as tennis from about 3 to 4 months after surgery
![Risiken]()
Risiken
Possible risks include general complications of surgery such as postoperative bleeding, infection, thrombosis, nerve injury (numbness, paralysis) and injury to vessels and soft tissue. Possible complications of this particular procedure include limited mobility of the knee joint, unsteadiness and pain (e.g., formation of painful, mechanically problematic scar tissue, non-healing of the meniscal suture, rupture of the sutured meniscal tear and rupture of the anchorage).
Removal of the torn meniscus
This is the most common arthroscopic procedure in the knee joint. If the meniscus is torn several times, if there are degenerative changes or if there is no blood supply to the torn areas, the tear cannot be sutured. This defective part of the meniscus, which no longer has a mechanical function, is removed following the principle of “as little as possible, as much as necessary”. When only the torn pieces of meniscus are removed it is known as a partial meniscal resection, and when the whole meniscus has to be removed it is known as a meniscal resection. This eliminates the annoying mechanical symptoms and the patient quickly becomes symptom-free.
As a result of this procedure, however, the load area of the residual meniscus becomes smaller, which can lead to it tearing in the event of overloading due to rotational movement. In addition, the absence of a portion of the meniscal buffer may lead to faster wear of the articular cartilage in the long term and thus to osteoarthritis of the knee. Suturing of the meniscus is attempted primarily for these reasons.
Facts and figures
![Operation]()
Operation
The procedure takes around 30 minutes
![Operation]()
Length of stay at the clinic
Performed on an outpatient basis in most cases
![After the treatment]()
After the treatment
Post-operative use of crutches to protect the knee for 1 to 2 weeks plus physiotherapy in exceptional cases
![Back to work]()
Back to work
No office work for 1 to 2 weeks, no strenuous physical activity for 4 to 8 weeks
![Sport]()
Sport
Knee-friendly sports such as swimming, cycling, fitness etc. from about 2 to 3 weeks after surgery; contact sports such as football or stop-and-go sports such as tennis from about 1 to 2 months after surgery
![Risks]()
Risks
Possible risks include general complications of surgery such as postoperative bleeding, infection, thrombosis, nerve injury (numbness, paralysis) and injury to vessels and soft tissue. Specific complications of this procedure include limited mobility of the knee joint, unsteadiness and pain (e.g., formation of painful, mechanically problematic scar tissue and additional tearing of the meniscus
Meniscus replacement
In very rare cases, the meniscus is not only removed but also replaced. This is primarily performed for younger patients with little or no cartilage damage. If the entire meniscus is affected, it can be replaced with a meniscal transplant using a donor meniscus. Biological tissue replacement is another option. The replacement meniscus is sutured into the defect. It consists of either collagen or polyurethane, which is gradually replaced by the body’s own tissue.
Our doctors have many years of experience and are highly skilled in sports and joint surgery. Dr Andreas L. Oberholzer is a well-known expert in knee surgery and has extensive experience in knee replacements. He trains international doctors in this area and supports the further development of soft-tissue-oriented techniques for the implantation of artificial knee joints. You can find out more about his work here.
We guarantee rapid, expert assessment and consultation and treatment in line with the latest medical findings. Don’t hesitate to get in touch if you would like a second opinion.